Nerve
conduction study is mainly used for the evaluation of paresthesia
(numbness, tingling, or burning sensation), weakness of the arms and
legs. This type of study is dependent on the part of limbs presented the
symptoms. A physical examination and thorough history also help to
direct the investigation. Some of the common disorders which we can
diagnose by the NCS are the following.
· Peripheral neuropathy (Median nerve, Ulnar nerve, Radial nerve, Peroneal nerve, Shoral nerve etc)
· Carpal tunnel syndrome (Median nerve compression)
· Guillain Barre syndrome (disease of peripheral nerves having numbness and weakness in limbs)
· Fascio – Scapulo – Humeral muscular dystrophy
· Spinal disc herniation

Components of NCS:
NCS has the following components.
- Motor NCS
- Sensory NCS
- F – wave
- H – reflex
A. Motor NCS:
Motor
NCS are performed by electrical stimulation of peripheral nerve and
recording from muscle supplied by that nerve. The time it takes for
electrical impulse to travel from the stimulation (electrode) of the
nerve to the recording electrode is called latency (ms). The size of the
response of the stimulation is called amplitude which is measured in
millivolt (mv). The nerve conduction velocity is determined from the
differences of the latencies on the two different locations and the
distance between the electrodes.


B. Sensory NCS:
Sensory
nerve conduction study are performed by the electrical stimulation of
the peripheral nerve and recording a purely sensory portion of the nerve
such as on finger i.e. the most distal portion of the limb. Recording
electrode will be proximal of the two electrodes (stimulatory electrode
is distal). Like the motor nerve conduction study, latency is measured
in millisecond (ms) while the amplitude is too low that can not be
measured in millivolts (mv) so it can be measured in microvolt (µv). The
nerve conduction velocity is calculated from the latency and the
distance between the electrodes i.e. nerve conduction velocity is
measured in m/s. This is called sensory nerve conduction study.


C. F – Wave study:
It
is the measured of time required for action potential of the motor
neuron elicited by applying a supramaximal stimulus (above the threshold
value) to the peripheral nerve that is to be transmitted to the
Anterior Horn Cells and return as a recurrent discharge along the same
nerve to activate the muscle that will be recorded by the recording
electrode.


The
latency of the F – wave response is approximately 22 – 34 ms in the
upper limb and 40 – 58 ms in the lower limb when they are stimulated at
the wrist and ankle respectively.
It
is the useful supplement to the NC and electromyography and is most
helpful in the diagnosis of condition where the most proximal portion of
the nerve is damaged like Guillain Barre Syndrome and Thoracic outlet
syndrome.
D. H – Reflex:
It
was first suggested by Hoffman and it is useful measurement for
rediculopathy and peripheral nerve pathy. It is the testing of both the
integrity of sensory and motor monosynaptic pathway of S1 nerve root to some extent for C6 and C7.
When a submaximal stimulus (below the threshold value) is applied to
the peripheral nerve, the action potential travel along afferent neuron
(I a) and synapse with the AHCs in the spinal cord. AHCs send
information along the motor neuron causing contraction of the muscle.

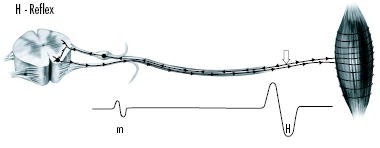
The H – reflex latency is the function of age and leg length.
H – Reflex latency = 0.46 (leg length in cm) + 9.14 + 0.1 (age in years)
Note: Stimulatory electrode should be placed on muscle belly and recording electrode should be placed on muscle origin.
The highly experienced team at Comprehensive Neurological Care Victoria includes Neurologists and a Neurophysiology Scientist. These specialist services are complimented by Neurophysiology diagnostic testing; EEG (Electroencephalography), NCS (Nerve Conduction Studies) and EMG (Electromyography)....Neurology Melbourne
ReplyDelete